⚠️ How to Use This Guide
This guide is for education only. It is not medical advice and does not replace your physician. Prostate cancer is serious. Before making any treatment decisions, work with a qualified urologist or oncologist. Everything in this guide — including alternative approaches — should be discussed with your doctor before you act on it.
That said: the more you know walking into that appointment, the better the conversation you'll have. That's why this page exists.
✅ First Steps Checklist
If you've just received a diagnosis or concerning lab result, do these in order:
- Get your PSA history in writing — a single PSA means little; the trend over time is what matters
- Obtain a copy of your biopsy pathology report — you have a legal right to it
- Ask specifically about transperineal biopsy before any procedure — see the critical callout below
- Understand your Gleason score / Grade Group before agreeing to any treatment
- Request an MRI (mpMRI) before biopsy if possible — MRI-guided fusion biopsy is more accurate
- Get a second opinion at an NCI-designated cancer center before any surgery or radiation
- Ask about active surveillance — for low-risk (Gleason 6/Grade Group 1) disease, this is the guideline-recommended option
- Ask specifically: "Is HoLEP available here?" — for BPH surgical candidates
- Review your medications — if on finasteride or dutasteride, read Part 3 before your next appointment
Part 1: Understanding Your Diagnosis
Is It BPH or Prostate Cancer? Or Both?
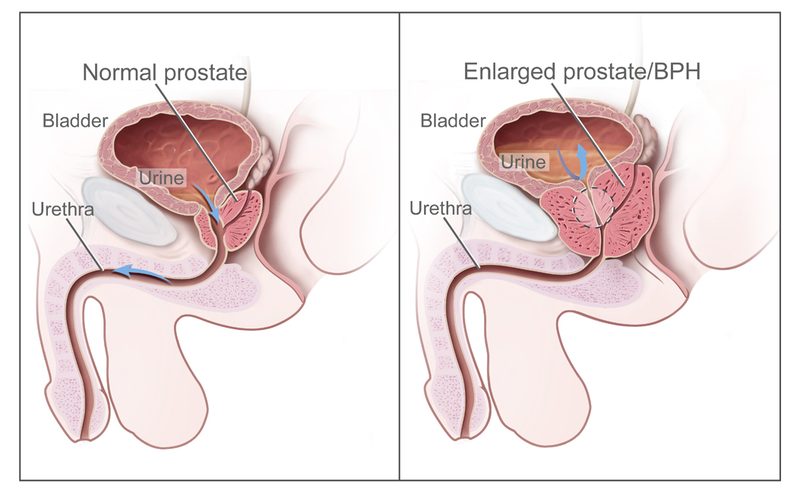
The prostate is a walnut-sized gland sitting directly below the bladder. It wraps around the urethra — which is why when it grows, it squeezes your urine stream like a thumb on a garden hose.
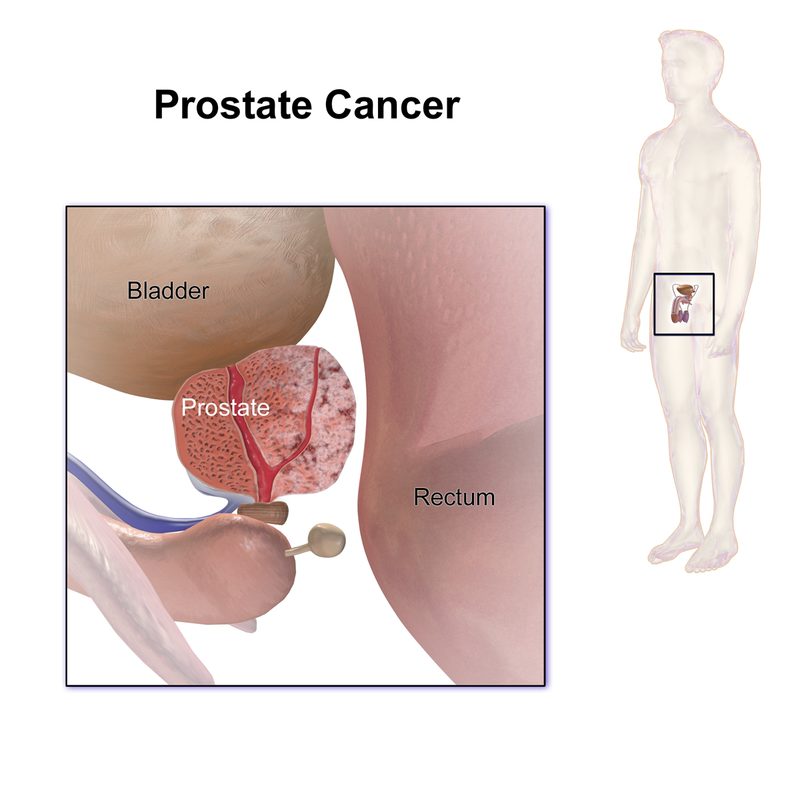
Two completely different problems can affect it:
BPH (Benign Prostatic Hyperplasia) — the prostate simply gets bigger with age. Not cancer. Not dangerous in itself, but it can make your life miserable: weak stream, getting up three times a night, feeling like you never fully empty. By age 60, roughly half of men have significant BPH. By age 85, about 90% do.
Prostate Cancer — abnormal cell growth within the prostate. The most commonly diagnosed cancer in American men (~288,000 new cases per year). Here's the critical nuance most patients aren't told: most prostate cancers are slow-growing and will never threaten your life. The challenge is distinguishing the slow ones from the fast ones — and the medical system often gets this wrong in the direction of overtreatment.
You can have both BPH and prostate cancer simultaneously — they're separate processes.
Understanding PSA: The Test That's Both Essential and Imperfect
PSA (Prostate-Specific Antigen) is a protein made by prostate cells. Here's what most patients don't know:
- PSA rises from many causes — BPH, prostatitis, recent ejaculation, vigorous cycling, even a DRE done just before the test
- "Normal" PSA is not a fixed number — 4.0 ng/mL is the old threshold; many experts now use age-adjusted ranges
- PSA velocity matters more than a single number — a rapid rise over months is more concerning than a stable elevated level
- A high PSA does not mean cancer. A "normal" PSA does not rule it out
The PSA Screening Controversy: The USPSTF long recommended against routine PSA screening because of overdiagnosis rates. When PSA screening dropped after 2012 guidance, late-stage prostate cancer diagnoses increased. Many experts believe the pendulum swung too far against screening. Our honest take: PSA screening makes sense for most men over 50, but what you do with the result requires careful, unhurried conversation.
Understanding Gleason Score and Grade Groups
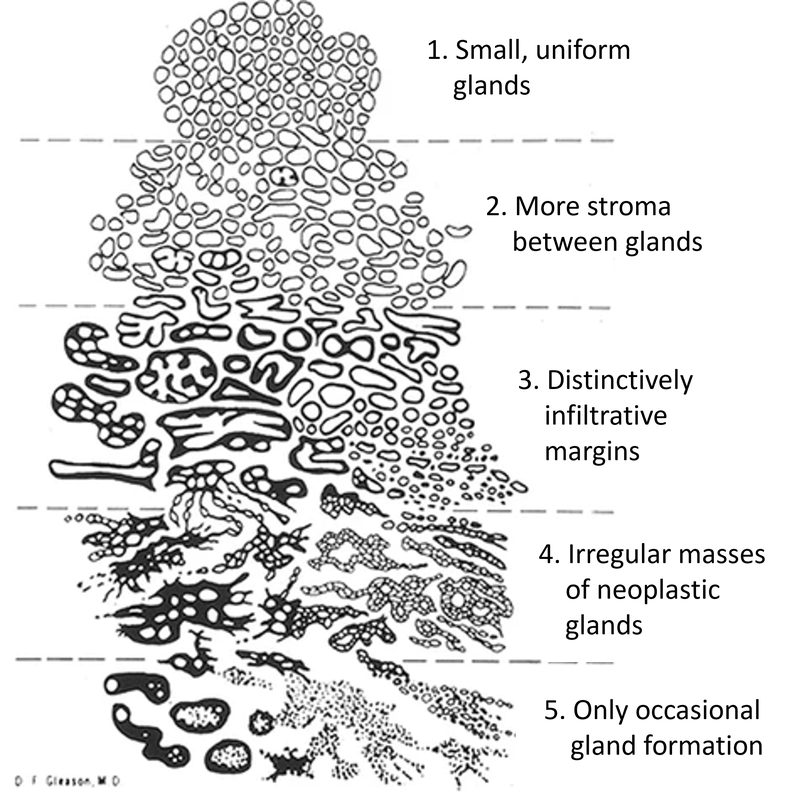
| Gleason Score | Grade Group | What It Means |
|---|---|---|
| 3+3 = 6 | Grade Group 1 | Low risk. Slow-growing. Strong evidence for active surveillance. |
| 3+4 = 7 | Grade Group 2 | Intermediate risk. Surveillance still possible for some. |
| 4+3 = 7 | Grade Group 3 | Intermediate-high risk. Treatment usually recommended. |
| 8 | Grade Group 4 | High risk. Treatment strongly recommended. |
| 9–10 | Grade Group 5 | Very high risk. Aggressive treatment recommended. |
The most important thing to know: A Gleason 6 (Grade Group 1) cancer has never been shown to metastasize in any clinical study when properly characterized. Yet historically, the majority of these men received immediate surgery or radiation. This is a major patient harm. Active surveillance is the guideline-recommended option for low-risk disease — but many patients are never offered it.
Clinical Staging (Plain English)
- Stage I–II: Cancer confined to the prostate. Highly treatable. 5-year survival near 100%.
- Stage III: Cancer has spread to nearby tissue but not distant organs.
- Stage IV: Cancer has spread to lymph nodes or distant organs (bones most commonly). Requires systemic treatment.
Part 2: Conventional Treatments
Section A: BPH Treatments
For mild-to-moderate symptoms, lifestyle changes first: reduce evening fluids, limit caffeine and alcohol, double-void technique, timed voiding, Kegel exercises. For many men, this is sufficient.
BPH Medications
Alpha Blockers (tamsulosin/Flomax, alfuzosin, doxazosin)
Relax smooth muscle in the prostate and bladder neck. Symptoms improve within days to weeks. They do not shrink the prostate — the underlying problem continues to grow. Side effects include dizziness, retrograde ejaculation, and rarely abnormal iris syndrome during cataract surgery. Tell your ophthalmologist before eye surgery if you've ever taken these.
⚠️ 5-Alpha Reductase Inhibitors (finasteride/Proscar, dutasteride/Avodart) — What Your Doctor May Not Tell You
Evidence rating: ⭐⭐⭐
These drugs block conversion of testosterone to DHT, shrinking the prostate 20–30% over 6–12 months. Side effects include erectile dysfunction, decreased libido, ejaculation disorders, gynecomastia, and in some men persistent sexual side effects even after stopping (Post-Finasteride Syndrome).
The FDA issued a Black Box Warning in 2011. Here's why: The landmark Prostate Cancer Prevention Trial (PCPT) found finasteride reduced prostate cancer incidence by 25% — but men who developed prostate cancer on finasteride were more likely to have high-grade (Gleason 7+) disease compared to placebo. The mechanism may be partly detection artifact, but the FDA warning stands.
If you're on finasteride or dutasteride, ask your doctor: "Is my Gleason score or biopsy interpretation being adjusted for the fact that I'm on a 5-ARI?"
🏆 HoLEP — The Mohs Surgery Moment for Your Prostate
Evidence rating: ⭐⭐⭐ (Multiple RCTs, AUA guideline recommendation)
If you know your skin cancer, you know that Mohs surgery is dramatically superior to standard excision for many skin cancers — but most dermatologists don't perform it because of the steep learning curve. Patients who don't know to ask never get it.
HoLEP (Holmium Laser Enucleation of the Prostate) is the same story for BPH surgery.
What the evidence actually shows:
- Complete tissue removal: HoLEP enucleates whole lobes of the prostate rather than chipping at it — removes more obstructing tissue than TURP, more completely, with less bleeding
- Works on any prostate size: TURP is limited to smaller prostates. HoLEP handles giant prostates (200g+) with no size limit
- Lower re-treatment rate: TURP re-treatment at 8 years: ~15%. HoLEP: significantly lower with 10+ year durable results
- Less bleeding: Preferred for men on blood thinners
- AUA recognition: The only BPH surgical option recommended for all prostate sizes
A published paper in PMC states: "HoLEP is bound to be the new gold standard for endoscopic treatment of BPH, the only remaining obstacle being the lack of mentorship and training."
Why doesn't every urologist offer it? Direct quote from Cleveland Clinic: "If a urologist doesn't learn HoLEP during residency or fellowship, the barriers to mastering the procedure are high." Estimated 30–50 cases needed for full competency. Most urologists trained on TURP aren't going back to learn.
What to do: Ask your urologist specifically: "Do you perform HoLEP? If not, can you refer me to someone who does?" Driving an extra hour to a major academic medical center is worth it.
Find HoLEP providers: Cleveland Clinic, Johns Hopkins, UCSF, Mayo Clinic, and most large university hospital urology departments.
TURP — Transurethral Resection of the Prostate ⭐⭐⭐
The "gold standard" that most urologists were trained on. A wire loop is inserted through the urethra and prostate tissue is shaved away. Significant symptom improvement in 85–90% of men. Side effects: retrograde ejaculation (75–90%), bleeding, re-treatment rate ~15% at 8 years. Still widely used largely because of training, not clinical superiority.
UroLift ⭐⭐⭐
Small implants hold prostate lobes apart. Best for moderate BPH (<80g, no large middle lobe) in men who want to preserve ejaculatory function. Does not cause retrograde ejaculation in most patients. Less durable than HoLEP — some patients need retreatment within 3–5 years.
Rezum — Water Vapor Therapy ⭐⭐⭐
Steam injected into prostate tissue causes cell death. Office procedure, local anesthesia. Retrograde ejaculation rate: approximately 5.3% — dramatically lower than TURP or HoLEP. Good for men prioritizing ejaculatory function preservation. Some temporary urinary retention expected in first 1–2 weeks. Good 4-year durability data.
Aquablation — Robotic Water Jet Therapy ⭐⭐⭐
Computer-guided high-velocity water jet ablates prostate tissue under real-time ultrasound guidance. Good for larger prostates (30–150g). WATER trial showed retrograde ejaculation rate of 10% vs. 36% for TURP. Erectile function largely preserved. Available at major academic centers.
Section B: Prostate Cancer Treatments
Active Surveillance — The Underutilized Right Answer
Evidence rating: ⭐⭐⭐ (Multiple large prospective cohort studies, guideline-supported)
50% of men diagnosed with prostate cancer have low-risk (Gleason 6 / Grade Group 1) disease. Multiple studies confirm Gleason 6 cancers virtually never metastasize when properly characterized. Yet for decades, the majority received surgery or radiation for a cancer that was never going to kill them.
Active surveillance is now the guideline-recommended approach for low-risk disease from ASCO, AUA, and NCCN.
Why is it still underutilized? A January 2025 study published in JAMA Network Open found a direct, statistically significant association between physician payment incentives and whether patients received active surveillance vs. immediate treatment. Urology practices that own radiation vaults have higher immediate treatment rates. When those practices divest from radiation equipment, treatment rates fall.
This is not a conspiracy theory. It's published data in JAMA.
What active surveillance involves: PSA every 3–6 months; MRI every 1–2 years; repeat biopsy at 6–12 months then every 1–3 years. 10–15 year cancer-specific survival on active surveillance for low-risk disease exceeds 99%.
If you have low-risk prostate cancer and your urologist schedules surgery or radiation without discussing active surveillance — get a second opinion.
Radical Prostatectomy (Surgery) ⭐⭐⭐
Surgical removal of the entire prostate. Robotic (da Vinci) is now the dominant approach. 5-year biochemical recurrence-free survival for localized disease: approximately 85–95%.
The side effects they may not fully prepare you for:
- Incontinence: In population-based studies, approximately 20% of men report some degree of urinary leakage at 12 months. Improves with pelvic floor exercises over 6–18 months for most.
- Erectile dysfunction: Published literature ranges 11–87% — almost entirely surgeon-dependent. In population-based cohorts, clinically significant ED at 18 months affects roughly 50–80% of men. May improve over 2–3 years with penile rehabilitation.
The honest conversation you deserve: Ask your surgeon: "What are YOUR personal 12-month continence and potency rates?" If they can't or won't answer, that's information.
Radiation Therapy Options ⭐⭐⭐
EBRT (External Beam Radiation Therapy): Modern versions include IMRT and IGRT. Multiple sessions over weeks.
SBRT / CyberKnife / SABR: High doses in 5 or fewer sessions. Outcomes comparable to conventional EBRT in well-designed trials for low-to-intermediate risk disease.
Brachytherapy (Seed Implants): Radioactive seeds implanted directly in the prostate. Excellent long-term outcomes for low-to-intermediate risk. No daily trips to a radiation center.
Proton Therapy: Theoretically less dose to surrounding tissues. Current evidence does not clearly demonstrate superior outcomes vs. photon-based IMRT for prostate cancer.
Side effects (honest): Bowel symptoms (urgency, rectal bleeding), urinary irritation, erectile dysfunction (develops more slowly than post-surgery). Late effects can appear years later.
Focal Therapy: HIFU, Cryotherapy ⭐⭐
Treat only the cancer-containing area of the prostate — preserving sexual and urinary function. FDA-approved since 2015. Good functional outcomes. Long-term comparative data vs. established treatments is still accumulating. Best at experienced centers with published outcomes.
Hormone Therapy (ADT) ⭐⭐⭐
ADT starves prostate cancer of testosterone. Used for high-risk localized disease (with radiation), recurrent disease, and metastatic disease. Side effects (the honest version): hot flashes, loss of libido, erectile dysfunction, fatigue, bone density loss, increased cardiovascular risk, metabolic syndrome, cognitive effects, depression, muscle loss, weight gain. These are not minor. ADT is often added in contexts where the evidence for benefit is marginal — particularly for low-risk disease. Second opinions matter.
🔔 NEW (March 2026): Oestradiol Patches as ADT Alternative — PATCH/STAMPEDE Trial
Finding (NEJM, March 29, 2026): For men with locally advanced prostate cancer requiring ADT, oestradiol patches (transdermal hormone therapy) are as effective as LHRH agonist injections (Lupron) — but with dramatically better tolerability.
The Evidence: A 1,360-patient randomized trial followed men for 3+ years with locally advanced, non-metastatic prostate cancer.
- Cancer control: 87% (patches) vs. 86% (injections) — essentially identical
- Hot flushes: 44% (patches) vs. 89% (injections) — oestradiol dramatically better tolerated
- Bone fractures at 5 years: 2.8% (patches) vs. 5.8% (injections) — significant bone protection advantage
- Breast swelling: 85% (patches) vs. 42% (injections) — this is the tradeoff
- Quality of life: Patches administered at home; injections require hospital/GP visits
Clinical significance: This is practice-changing for locally advanced disease. Men can now choose between injections and patches based on their side-effect tolerance. The patches are currently off-label for prostate cancer (approved for menopausal HRT), but NEJM publication is accelerating licensing discussions with manufacturers for prostate-specific indication.
Ask your oncologist: "Are oestradiol patches available as an ADT option for my case? If my priority is reducing hot flushes and bone fractures, what's the pathway to access?"
Advanced / Metastatic Disease Options ⭐⭐⭐
- Enzalutamide / Apalutamide / Darolutamide: Next-generation anti-androgens with significant survival benefit
- PARP inhibitors (olaparib, rucaparib): For men with BRCA1/2 or other DNA repair gene mutations — get genetic testing if you have high-risk or metastatic disease
- 177Lu-PSMA-617 (Pluvicto): FDA-approved 2022 — radioligand therapy targeting PSMA-expressing cancer cells. A major recent advance. Get PSMA PET/CT scan if metastatic.
- Pembrolizumab: For MSI-H/dMMR tumors — get tumor molecular profiling
- Radium-223 (Xofigo): Targets bone metastases, extends survival. 🔔 NEW DATA (March 2026): PEACE-3 trial long-term results show that combining enzalutamide + radium-223 + bone protective agent (Prolia/Xgeva) for metastatic castration-resistant prostate cancer (mCRPC) with bone metastases achieves 24% reduction in mortality compared to enzalutamide alone — a practice-changing result. Radiographic progression or death reduced 29%. Critical: bone protective agent is mandatory to prevent fractures.
- 🔔 NEW (March 2026): VIR-5500 — Early-stage trial results show "stunning" immunotherapy response in advanced prostate cancer. Monoclonal antibody approach. Ask your oncologist about clinical trial availability. Promising results reported by The Guardian (Feb 28, 2026). Monitor for Phase II/III trial openings.
Part 3: What Your Doctor Probably Didn't Mention
Important: The treatments and interventions below range from well-researched to emerging to lifestyle-based. We rate the evidence honestly. None of this constitutes a treatment recommendation. Discuss everything with your physician before acting on it.
🔴 Critical: The Biopsy Route Your Doctor May Not Have Offered You
Transperineal vs. Transrectal Biopsy — This Is Not a Minor Decision
Evidence rating: ⭐⭐⭐ (TRANSLATE RCT, Lancet Oncology 2025)
Transrectal (TRUS-guided): The traditional approach. Needle passes through the rectal wall into the prostate. Sepsis risk: 1–2% of patients.
Transperineal: Needle passes through the skin between the scrotum and anus — not through the rectum. Standard of care in the UK, Australia, and much of Europe. Still not routine in the US.
The 2025 TRANSLATE trial (Lancet Oncology): Switching from transrectal to transperineal "eliminates sepsis as a complication." The transperineal sepsis rate: approximately 0.002% — roughly 500x lower than transrectal.
Needle track seeding: A biopsy needle passing through cancerous tissue can theoretically deposit cancer cells along the needle track. With transrectal biopsy, any seeding occurs inside the rectum — making later salvage surgery significantly more complex. Transperineal seeding, if it occurs, is in far more surgically accessible tissue.
Better cancer detection: Transperineal provides better access to the anterior prostate (a region often missed by transrectal needles), resulting in higher detection rates of clinically significant cancer.
Ask your urologist: "Do you offer transperineal biopsy? If not, can you refer me to someone who does?" The fact that most US urologists still default to transrectal is a training and infrastructure issue, not a clinical one.
🥦 Sulforaphane (Broccoli Sprouts) — The Cheap Intervention With Real Data ⭐⭐⭐
If nicotinamide is the overlooked cheap intervention for skin cancer prevention, sulforaphane from broccoli sprouts is its equivalent for prostate cancer.
Sulforaphane is produced when cruciferous vegetables are chewed — most abundantly in broccoli sprouts, which contain 10–100x more sulforaphane than mature broccoli.
Animal studies: In TRAMP transgenic mice (the gold-standard prostate cancer animal model), a 15% broccoli sprout diet reduced adenocarcinoma incidence from 89% to 37%.
Human RCT — ESCAPE trial (2019): A 12-month randomized, placebo-controlled trial of glucoraphanin-rich broccoli powder in men with low-risk prostate cancer on active surveillance showed significant transcriptional changes in prostate tissue — measurable alterations in gene expression pathways associated with cancer progression.
Mechanisms: Activates the Nrf2 pathway, promotes cancer cell apoptosis, inhibits HDAC (epigenetic regulation), reduces NF-κB inflammatory signaling — multiple independent anti-cancer pathways.
Practical: Eat broccoli sprouts (2–3 tablespoons daily), or supplement with sulforaphane standardized to glucoraphanin. Sprouts are preferable — processing affects bioavailability.
Sulforaphane broccoli sprout supplement → Buy on Amazon
Discuss with your physician before using high-dose supplements.
🥛 The Dairy-Prostate Connection: What Dietary Guidelines Aren't Telling Men ⭐⭐⭐
This is one of the most important, least-discussed findings in prostate cancer epidemiology — and a core insight in Ben Ong's All About The Prostate.
The Harvard Physicians' Health Study: Dairy products and calcium associated with greater risk of prostate cancer. Proposed mechanism: high calcium intake from dairy suppresses circulating levels of 1,25-dihydroxyvitamin D — the active form of Vitamin D that protects against prostate cancer.
The IGF-1 pathway: High dairy intake elevates circulating insulin-like growth factor 1 (IGF-1) — a potent growth factor directly implicated in prostate cancer progression.
The meta-analysis: A 2016 meta-analysis combining 11 studies found that men consuming the most dairy products had a 43% higher risk of dying of prostate cancer compared to men who largely avoided dairy.
The three mechanisms:
- High calcium from dairy suppresses protective 1,25-vitamin D₃
- Milk consumption raises IGF-1, promoting cancer cell proliferation
- Commercial dairy from pregnant cows contains significant estrogen — potential endocrine disruption
Why your doctor may not have mentioned this: Dairy industry influence on dietary guidelines is well-documented. There's no commercial sponsor funding physician education on this — no drug to sell.
📖 Ben Ong's Natural Prostate Protocol
About Ben Ong: Author of All About The Prostate: The Definitive Guide to Healing Your Prostate Naturally (11th edition). Ben suffered from prostate disease himself in 2000 and spent two decades researching natural interventions.
Foods to Avoid (Evidence-Supported)
- Dairy — see section above ⭐⭐⭐
- Refined sugars and processed carbohydrates — drive insulin/IGF-1 elevation; inflammatory
- Alcohol — worsens BPH symptoms; associated with prostate irritation
- Red and processed meat — epidemiological associations with prostate cancer risk
Foods to Prioritize
- Broccoli sprouts / cruciferous vegetables — sulforaphane ⭐⭐⭐
- Cooked tomatoes/tomato products — lycopene ⭐⭐
- Pumpkin seeds — zinc, phytosterols ⭐⭐
- Fatty fish (salmon, sardines) — omega-3s, anti-inflammatory
- Green tea — EGCG ⭐⭐
- Extra virgin olive oil — anti-inflammatory polyphenols
Exercise Protocol ⭐⭐⭐
The Harvard Health Professionals Follow-Up Study found that men who were more physically active were significantly less likely to suffer from BPH. Walking an extra 3 hours per week was associated with a 10% reduction in BPH risk. Post-diagnosis physical activity also reduces prostate cancer progression risk. Brisk walking in particular showed anti-proliferative effects — serum from exercising men suppressed prostate cancer cell growth in vitro.
- Brisk walking 30+ min/day ⭐⭐⭐
- Resistance training 2–3x/week ⭐⭐ — maintains testosterone balance, preserves muscle during ADT
- Pelvic floor exercises (Kegels) ⭐⭐⭐ — proven for continence after prostatectomy; also helps BPH
Available at: Ben Ong's book on Amazon → Buy on Amazon and bensnaturalhealth.com
Lycopene (Cooked Tomatoes) ⭐⭐
The Harvard Health Professionals Follow-Up Study (47,000+ men) found frequent tomato/tomato product intake was associated with reduced risk of prostate cancer. Bioavailability is actually higher in cooked/processed tomato products. Preclinical data shows lycopene inhibits prostate cancer cell growth. Daily serving of tomato-based food is a zero-downside recommendation. Discuss with your physician before supplementing.
Green Tea / EGCG ⭐⭐
An NCI randomized trial of Polyphenon E (400mg EGCG) showed statistically significant reductions in serum PSA and other biomarkers in men with high-grade PIN. An Italian RCT showed green tea catechins (600mg/day) reduced prostate cancer incidence in men with HGPIN from 30% (placebo) to 3% over one year. A 2023 meta-analysis of 14 RCTs supports a protective effect. Practical: 3–4 cups daily or 400–600mg EGCG supplement. Discuss with physician if on blood thinners.
Pomegranate Juice ⭐⭐ (Phase II) / ⭐ (Phase III)
The initial UCLA Phase II trial was eye-catching — PSA doubling time extended from 15 to 54 months. The Phase III randomized, placebo-controlled trial was a cold shower: pomegranate extract did not significantly prolong PSA doubling time vs. placebo. Both arms showed improvement — suggesting a strong placebo effect in the Phase II trial. Honest take: as a healthy food, reasonable inclusion in a prostate-health diet. Not a primary intervention.
Vitamin D ⭐⭐
Multiple observational studies link Vitamin D deficiency to increased prostate cancer aggressiveness and mortality. Cedars-Sinai research (2024) found Vitamin D deficiency may explain why African American men experience more aggressive prostate cancer at younger ages. Importantly: high dairy/calcium intake suppresses the active form of Vitamin D — connecting the dairy-prostate link to the Vitamin D mechanism. Get your 25-OH vitamin D tested. Correct deficiency. Discuss supplementation with your physician — the relationship between high-normal levels and prostate cancer is complex.
Beta-Sitosterol (For BPH) ⭐⭐⭐
A Cochrane Systematic Review found beta-sitosterol improved urinary symptom scores and flow measures in men with BPH vs. placebo. Found in saw palmetto, pumpkin seeds, and many plant foods. This may explain some of saw palmetto's observed benefit in earlier studies. Discuss with your physician before supplementing.
Pumpkin Seed / Oil (For BPH) ⭐⭐
The 2014 GRANU trial — a 1-year, randomized, placebo-controlled study — found 12 months of pumpkin seed treatment led to clinically relevant reduction in IPSS vs. placebo. A second RCT compared pumpkin seed oil against tamsulosin (Flomax) and found clinically meaningful improvement. Rich in zinc, phytosterols, and anti-inflammatory compounds. Discuss with your physician before supplementing.
Saw Palmetto — The Honest Assessment ⭐
The most popular supplement for BPH. Earlier studies and a 1998 JAMA meta-analysis were promising. However: the 2006 STEP trial published in the New England Journal of Medicine found saw palmetto extract "did not reduce urinary symptoms associated with BPH more than placebo" even at triple the standard dose. A 2011 follow-up confirmed no benefit. We can't recommend it as a primary intervention based on current best evidence. The beta-sitosterol it contains (which does have evidence) may explain some of the earlier positive results.
📖 Want the Complete Prostate Protocol?
"Prostate Health: What Your Urologist May Not Tell You"
The full guide — HoLEP vs TURP in detail, the complete natural protocol, the dairy bombshell, the biopsy route that eliminates sepsis, active surveillance decision framework, and Ben Ong's full dietary protocol. 12,000+ words, 8 chapters, evidence-rated throughout.
Instant download. No subscription.
Part 4: Clinical Trials
Clinical trials are how medicine improves — and for men with advanced or recurrent prostate cancer, a trial may offer access to treatments years before FDA approval.
Where to find trials:
- ClinicalTrials.gov — search "prostate cancer" + your stage/treatment history
- Prostate Cancer Foundation (PCF) — curated trial navigator
- National Cancer Institute
Currently active areas of promise: PSMA-targeted therapies, PARP inhibitors in HR-deficient cancer, combination ADT + novel anti-androgens, immunotherapy combinations, AR splice variant targeting.
Part 5: Getting a Second Opinion
For BPH Surgery
Before any BPH surgical procedure, ask specifically whether a HoLEP-trained surgeon is available. High-volume HoLEP centers include: Cleveland Clinic, Johns Hopkins Urology, UCSF Urology, Mayo Clinic, Northwestern Memorial Hospital, and University of Washington Medical Center.
For Prostate Cancer
For any cancer diagnosis above Grade Group 1, a second opinion at an NCI-designated Comprehensive Cancer Center is worth the trip:
- Memorial Sloan Kettering Cancer Center (New York)
- MD Anderson Cancer Center (Houston)
- Johns Hopkins Medicine (Baltimore) — particularly active surveillance
- UCSF — leading active surveillance program
- Stanford Cancer Institute
- Mayo Clinic (Rochester, Phoenix, Jacksonville)
- Cleveland Clinic Taussig Cancer Institute
Part 6: Questions to Ask Your Doctor
Print this. Bring it to your appointment.
For BPH Evaluation
- "What is my prostate volume and IPSS score — and what do they mean for treatment options?"
- "Do you offer HoLEP? If not, can you refer me to a HoLEP surgeon?"
- "If I'm on a 5-alpha reductase inhibitor, what does the FDA black box warning mean for me?"
- "What's your personal re-treatment rate for the procedure you're recommending?"
- "What happens if I choose watchful waiting?"
For Biopsy
- "Do you offer transperineal biopsy?" (If not: ask for a referral)
- "Would an MRI first (mpMRI) help target the biopsy and reduce unnecessary cores?"
- "What is the infection risk with the approach you recommend?"
For Prostate Cancer Diagnosis
- "Is my Gleason score/Grade Group appropriate for active surveillance?"
- "What is your active surveillance program — exactly what monitoring schedule?"
- "Is my biopsy interpretation affected by being on a 5-alpha reductase inhibitor?"
- "What are YOUR personal incontinence and erectile dysfunction rates at 12 months?" (Ask the surgeon directly)
- "Should I get genomic tumor testing (Oncotype DX, Decipher, Prolaris) before deciding?"
- "Should I get genetic testing (BRCA1/2, ATM, CHEK2)?"
- "Are there clinical trials I qualify for?"
- "What is the evidence that immediate treatment is better than active surveillance for MY specific case?"
Part 7: Prevention & Ongoing Monitoring
Diet
- Reduce or eliminate dairy ⭐⭐⭐
- Eat cooked tomatoes/lycopene daily ⭐⭐
- Eat broccoli/cruciferous vegetables regularly ⭐⭐⭐
- Green tea daily ⭐⭐
- Anti-inflammatory dietary pattern ⭐⭐
- Reduce refined sugar and processed foods ⭐⭐
- Limit red and processed meat ⭐⭐
Supplements With Reasonable Evidence
- Vitamin D (optimize levels) ⭐⭐
- Zinc (pumpkin seeds or supplement) ⭐⭐
- Beta-sitosterol (for BPH) ⭐⭐⭐
- EGCG/green tea catechins ⭐⭐
Discuss all supplements with your physician before starting.
Exercise
- 30–60 minutes brisk walking daily ⭐⭐⭐
- Resistance training 2–3x/week ⭐⭐
- Maintain healthy weight — obesity associated with more aggressive prostate cancer ⭐⭐⭐
PSA Screening
- Annual PSA starting at age 50 (or 40 for African Americans and men with first-degree relative with prostate cancer)
- Track your PSA trend — a single number is less meaningful than the trajectory
- Free PSA ratio can help distinguish cancer from BPH
- 🔔 PARADIGM SHIFT (March 2026): Research presented at the European Association of Urology Congress (EAU26) now shows prostate cancer screening effectiveness is equivalent to breast cancer screening. For decades, major health bodies recommended breast cancer screening while advising against prostate screening — a contradiction that is no longer defensible. If screening makes sense for one, it makes sense for both. Ask your doctor about screening options. Source: European Association of Urology Congress, March 2026; European Urology journal
🔔 NEW (March 2026): Cardiovascular Risk Considerations in ADT — Choose Your Antagonist Wisely
Finding (ASCO Genitourinary Cancers Symposium, March 2026): For men requiring ADT, your choice of medication affects cardiovascular risk. New data shows ADT antagonists (Degarelix, Relugolix) have significantly lower cardiovascular risk than agonists (Lupron/leuprolide).
The Evidence: Claims database analysis of real-world ADT initiation patterns found:
- Antagonists reduce major adverse cardiac events (MACE) — heart attack, non-fatal stroke — compared to agonists
- Greatest benefit in men with baseline cardiovascular disease — if you have a history of heart disease, hypertension, or other cardiac risk factors, antagonists should be preferred
- Relugolix (oral antagonist) is emerging as the safer alternative to Lupron for men with cardiac concerns
- Mechanism: Agonists cause an initial "flare" in testosterone before suppression (explaining some cardiovascular risk). Antagonists block testosterone immediately without flare.
What this means for you: If you're facing ADT for prostate cancer AND you have cardiovascular risk factors or a cardiac history, ask your oncologist specifically: "Would an ADT antagonist (Degarelix or Relugolix) be safer for my case than a Lupron agonist?" This is a personalized risk-benefit discussion worth having upfront.
Why this matters: ADT side effects include bone loss, metabolic syndrome, and cardiovascular risk. For men over 50 (Dave's demographic), cardiac safety should be part of the ADT decision. Don't assume all ADTs are equivalent — the class of drug matters.
Part 8: Patient Communities
- Prostate Cancer Foundation (PCF) — pcf.org
- ZERO — The End of Prostate Cancer — zerocancer.org
- Us TOO International — ustoo.org
- Active Surveillance Patients International (ASPI) — aspinternational.org
- Ben's Natural Health Community — bensnaturalhealth.com/blog
- Inspire Prostate Cancer Forum — inspire.com
Don't Let This Be the Last Thing You Learn
Join thousands of men who get our weekly prostate health research update — the findings that don't make it into mainstream medical news.
No spam. Unsubscribe anytime. We are not affiliated with any pharmaceutical company or treatment provider.
Why This Page Exists
Men facing BPH are routinely steered toward TURP — a 1960s procedure — when HoLEP has been demonstrated superior in the literature for decades. The reason? Training barriers and institutional inertia. Nobody is hiding this from you deliberately. But nobody is urgently telling you either.
Men with low-risk prostate cancer are still receiving surgery and radiation at alarming rates — procedures that carry real risks of incontinence and erectile dysfunction — for cancers that may never threaten their lives. A 2025 study in JAMA Network Open found physician payment incentives directly influence this. That's published peer-reviewed data.
And the dietary connections — dairy and prostate cancer, sulforaphane and prostate tissue gene expression, exercise and BPH risk — are sitting in the medical literature, not discussed in 15-minute appointments.
PlanetCure exists to close that gap. We're funded by our readers, not by pharmaceutical advertisers. We have no financial interest in which treatment you choose. We just want you walking into that appointment knowing what to ask.
Stay Informed
New research added regularly. Get notified when we update this page or publish new condition guides.
We will never sell your email. Not affiliated with any pharmaceutical company or treatment provider.
Disclosure: Some links on this page are Amazon affiliate links. If you purchase through these links, PlanetCure may earn a small commission at no additional cost to you. This does not influence our recommendations — we only link to products mentioned because of their evidence base, not for commercial reasons.
The content on this page is for informational and educational purposes only. It does not constitute medical advice, diagnosis, or treatment recommendations. Individual results vary and no treatment is effective for every patient or every diagnosis. Always consult a qualified, licensed healthcare professional before making any medical decision. PlanetCure is not affiliated with any pharmaceutical company, hospital system, or treatment provider, and does not receive compensation for the treatments or products mentioned on this page except where explicitly noted as affiliate links. Evidence ratings represent the editors' honest assessment of research quality and are intended to help readers calibrate confidence — not replace physician judgment.