This page is not medical advice. We are not your doctor. We are not affiliated with any pharmaceutical company, hospital system, or treatment provider. What we are is a research resource — the most complete one we could build — so that when you sit down with your doctor, or go find a better one, you know exactly what questions to ask.
Because informed patients get better outcomes. Every time.
Before You Read Any Further
This guide is for informational purposes only. It does not constitute medical advice and should not replace consultation with a qualified healthcare professional. Skin cancer treatment decisions should always be made in partnership with a licensed physician who knows your specific diagnosis, stage, and medical history.
What this guide does: catalogs every treatment option we could find, rates the evidence honestly, and helps you walk into your next medical appointment as an informed patient.
Some options here have strong clinical trial data. Some have emerging evidence. Some have patient community consensus and minimal formal research. We tell you which is which. We never claim anything works for everyone — because nothing does.
Read this. Then talk to your doctor.
Your First 7 Days: What to Do Before You Decide Anything
Most skin cancers are not emergencies. You have time to make a good decision. Use it.
- Get a copy of your pathology report. You're legally entitled to it. Ask for it today.
- Write down your exact diagnosis: type, stage, location, and whether margins were clear.
- Do NOT schedule surgery until you've read this entire page and consulted with at least one specialist.
- Ask your doctor: "Am I a candidate for Mohs surgery?"
- Ask your doctor: "Are there any clinical trials I qualify for?"
- Contact at least one major cancer center for a second opinion. Most offer remote consultations.
- Join a patient community. Real patients who've been exactly where you are right now.
- Start a folder — physical or digital — for every record, photo, and test result from this point forward.
Understanding What You Have
Before you can have an informed conversation about treatment, you need to understand exactly what you're dealing with. Here's what the different types of skin cancer actually mean — in plain English.
Basal Cell Carcinoma (BCC)
The most common skin cancer in the world. Over 3 million Americans are diagnosed every year.
The good news: BCC almost never spreads to other parts of the body. It grows slowly, stays local, and is highly treatable when caught — which it usually is.
The less-good news: it can cause real tissue damage if ignored, especially on the face. And it has a habit of coming back at the same site if not fully removed.
What it looks like: a pearly or waxy bump, a flat flesh-colored scar, a pink growth, or an open sore that heals and returns.

Bottom line: Highly treatable. Don't panic. Do take it seriously.
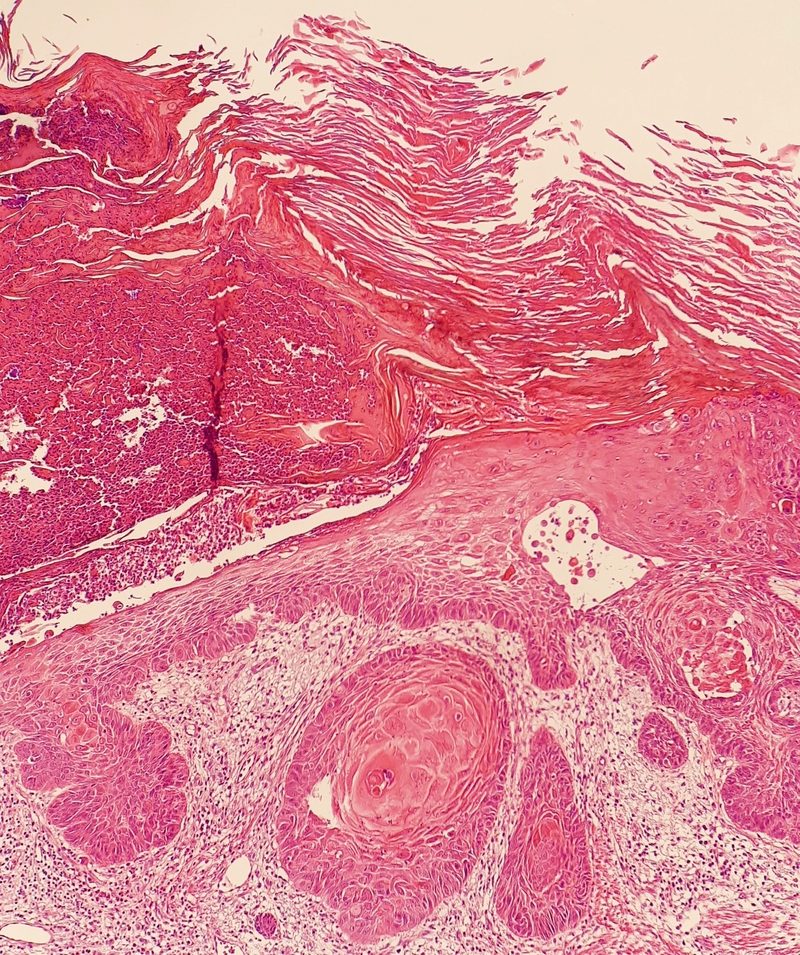
Squamous Cell Carcinoma (SCC)
Second most common skin cancer. About 1 million new cases in the US per year.
SCC is more aggressive than BCC — it can spread to lymph nodes and other organs if left untreated, though this only happens in approximately 2-5% of typical cases. That risk increases in immunocompromised patients and for cancers located on the lip, ear, or scalp.
What it looks like: a firm red nodule, a flat lesion with a scaly crust, a new sore on an old scar.
Bottom line: Treat it, and treat it properly. Discuss all available options with a qualified dermatologist or oncologist before proceeding.
Melanoma
Melanoma accounts for approximately 75% of all skin cancer deaths, even though it's far less common than BCC or SCC.
The reason melanoma is dangerous isn't that it's untreatable — it's that it can spread rapidly if not caught early. Early-stage melanoma (Stage 1) carries a 5-year survival rate of approximately 99%. Distant metastasis (Stage 4) drops to around 32%. That gap is why early detection and accurate staging are critical.

Important note: Immunotherapy has completely transformed melanoma treatment over the last decade. Patients with advanced melanoma should seek care at a major cancer center with a dedicated melanoma program. This is not a disease to manage with a general practitioner alone.
Merkel Cell Carcinoma (MCC)
Rare and aggressive — frequently misdiagnosed. MCC spreads quickly to lymph nodes. If this is your diagnosis, seek care at a major cancer center immediately. Immunotherapy has shown remarkable response rates for MCC in recent years.
Reading Your Pathology Report
Your pathology report is the foundational document for all treatment decisions. Key terms:
- Clear / Negative margins — the cancer was fully removed with clean borders. Good.
- Positive margins — cancer cells were found at the edge of removed tissue. Additional treatment is needed.
- Breslow thickness (melanoma) — depth of invasion in millimeters. Lower is better.
- Mitotic rate (melanoma) — speed of cell division. Higher indicates more aggressive behavior.
- Perineural invasion — cancer growing along nerve pathways. Affects treatment planning.
- Lymphovascular invasion — spread into blood or lymph vessels. Increases risk of distant spread.
If any terms in your report are unclear, ask your physician to explain them before making any treatment decision.
Conventional Treatment Options
These are established, medically recognized treatments. All have clinical evidence supporting their use. The right option for you depends on your specific diagnosis, stage, and location — which is why physician consultation is essential before choosing any path.
Mohs Micrographic Surgery
The gold standard that many patients are never offered
Standard excision — cutting out the tumor and stitching it up — is not always the most effective option. For BCC and SCC on the face, ears, nose, lips, hands, or genitals, Mohs surgery typically offers significantly better cure rates and smaller scars. Many general dermatologists don't perform Mohs and may not proactively recommend it. Asking specifically about it could meaningfully change your outcome.
In Mohs surgery, the tumor is removed one thin layer at a time. Each layer is examined under a microscope before the next is removed. Only tissue that tests positive for cancer is taken. Nothing more.
Published cure rates: 99% for primary BCC; 97% for recurrent BCC.
Ask your doctor: "Should I see a Mohs surgeon before deciding on treatment?"
Find a Mohs surgeon: mohscollege.org/find-a-surgeon
Standard Excision
The most common treatment: the tumor plus a margin of healthy tissue is surgically removed and the wound is stitched closed. Cure rates are approximately 90-95% for primary tumors. Appropriate for many diagnoses, though not always the optimal choice for high-risk locations or recurrent disease.
Cryotherapy
Liquid nitrogen freezes and destroys cancer cells. Fast and widely available. Best for superficial lesions, actinic keratoses, and early-stage BCC/SCC. Not appropriate for deeper or larger tumors.
Electrodesiccation & Curettage (ED&C)
The tumor is scraped and burned. Typically repeated 2-3 times in one session. Approximately 95% cure rate for appropriate (low-risk, superficial) lesions. Not recommended for high-risk locations or deeper tumors.
Image-Guided Superficial Radiotherapy (IG-SRT)
A surgery-free option most patients are never told about
Surgery is not the only medically established option for BCC and SCC. A published analysis of 2,917 lesions (PMC8140015) found that Image-Guided SRT had cure rates comparable to — and in some analyses superior to — surgery. Recent 2026 validation (Oncology and Therapy journal, March 2026) confirms superior outcomes at lower cost using adaptive radiotherapy protocols. No cutting. No stitching. No surgical scar. This treatment exists, it's covered by most insurance, and many dermatologists simply don't offer it or mention it.
IG-SRT uses precisely targeted low-level X-ray energy to destroy skin cancer cells. Administered in a dermatologist's office over approximately 15-20 sessions across 5 weeks.
Particularly appropriate for patients on blood thinners, older patients where surgery carries greater risk, and cosmetically sensitive locations.
Find an IG-SRT provider: gentlecure.com
Photodynamic Therapy (PDT)
A photosensitizing drug (aminolevulinic acid) is applied to the skin and absorbed preferentially by cancer cells. When activated by specific wavelengths of light, it selectively destroys those cells while sparing healthy tissue.
FDA-approved for actinic keratoses. Used off-label for superficial BCC and SCC. No surgical scarring; can treat large surface areas. Ask your dermatologist whether your specific lesion type is a candidate.
Prescription Topicals
Imiquimod (Aldara/Zyclara) — immune response modifier. FDA-approved for superficial BCC and actinic keratoses. Applied daily for 6-12 weeks. Approximately 80-85% clearance rate for appropriate lesion types. Causes local reaction (redness, crusting) — this is expected and indicates the medication is working.
5-Fluorouracil / 5-FU (Efudex, Carac) — topical chemotherapy. FDA-approved for actinic keratoses; used off-label for superficial BCC. Similar efficacy profile to imiquimod.
Both are legitimate alternatives to surgery for the right diagnosis. Ask your dermatologist specifically whether your lesion type and location are appropriate candidates.
Immunotherapy
For advanced or metastatic disease — this has changed outcomes dramatically
PD-1 inhibitors including pembrolizumab (Keytruda), nivolumab (Opdivo), and cemiplimab (Libtayo) have transformed treatment for advanced melanoma, advanced SCC, and advanced BCC. Five-year survival rates for Stage 4 melanoma have increased from under 10% to over 40% since these drugs became available.
These are complex treatments with significant potential side effects. They require management by an oncologist experienced with immunotherapy, ideally at a major cancer center.
Targeted Therapy (BRAF-Mutated Melanoma)
Approximately 50% of melanomas carry a BRAF V600E or V600K mutation. If yours does, BRAF and MEK inhibitor combinations (dabrafenib + trametinib; vemurafenib + cobimetinib) are available and can produce dramatic initial responses.
Ask about BRAF mutation testing if you have a melanoma diagnosis. It's a standard tissue test that determines whether these drugs are relevant for your case.
What Your Doctor May Not Have Mentioned
A note before you read this section:
The treatments below range from well-researched options that are simply underutilized, to approaches with emerging evidence, to options used primarily within patient communities with minimal formal clinical data.
We present all of them because we believe you have a right to know they exist. We rate the evidence honestly. We flag the risks clearly.
None of the information in this section constitutes a treatment recommendation. Do not use any of these approaches — particularly as a primary or sole treatment — without first consulting a qualified physician or integrative oncologist. Some of these options carry real risks if used incorrectly or in the wrong clinical situation. The evidence ratings below exist precisely so you can see what's proven, what's promising, and what's speculative.
Use this section to have a better conversation with your doctor. Not to self-treat.
Evidence ratings used throughout:
Perhaps the most important thing on this page
A Phase 3 randomized controlled trial published in the New England Journal of Medicine found that oral nicotinamide (500mg twice daily) reduced new basal cell and squamous cell cancer diagnoses by 23% compared to placebo.
A 2025 cohort study published in JAMA Dermatology found a 54% reduced risk of new skin cancer in patients with prior skin cancer history who took nicotinamide.
Nicotinamide — also called niacinamide — is a form of vitamin B3. It costs approximately $10-15 per month over the counter without a prescription.
The evidence is in peer-reviewed literature. The cost is negligible. Most dermatologists do not mention it.
What it does: Enhances DNA repair mechanisms and reduces UV-induced immunosuppression at the cellular level.
Dose used in studies: 500mg twice daily. This is niacinamide/nicotinamide — not regular niacin, which works differently and causes flushing. Look for "Niacinamide 500mg" at any pharmacy.
Who it's relevant for: Patients with a history of BCC or SCC who want to reduce the risk of developing new lesions. The published evidence is specifically for non-melanoma skin cancer chemoprevention in high-risk patients.
Peer-reviewed data. Outperformed a prescription cream. Almost unknown.
DMSO (dimethyl sulfoxide) penetrates skin deeply and carries other molecules with it. Combined with high-concentration vitamin C, it can deliver ascorbic acid directly to cancer cells.
A 2022 randomized controlled trial (ScienceDirect) found topical ascorbic acid in DMSO was superior at 8 weeks — and equally effective at 12 weeks — compared to imiquimod for low-risk superficial BCC, with fewer side effects. A 2025 preprint study showed promising results for squamous cell carcinoma in situ.
This is published, peer-reviewed data. It is not experimental fringe. It is simply not profitable to promote.
How it's used: 30% ascorbic acid dissolved in pharmaceutical-grade DMSO, applied topically to the lesion daily, with the lesion kept covered between applications.
Where to source: Pharmaceutical-grade DMSO is available OTC. Some integrative pharmacies will prepare the combination. DMSO (pharmaceutical grade) → Buy on Amazon
Used clinically in the UK. Peer-reviewed publications. Available internationally.
Curaderm BEC5 is a topical cream derived from solasodine glycosides — compounds found in eggplant and related plants. The active ingredient appears to selectively bind receptors overexpressed on cancer cells, triggering apoptosis (programmed cell death) while leaving normal cells less affected.
Multiple publications in indexed peer-reviewed journals document effectiveness against BCC and SCC, including a study in the Journal of Cancer Therapy and publications on PubMed.
Treatment profile: Applied daily to the lesion, kept covered. The lesion will react visibly — crusting and discharge are expected and indicate the treatment is working. Full treatment typically requires 8-12+ weeks.
Best for: Non-melanoma skin cancers — BCC, SCC, actinic keratoses.
Not recommended for: Melanoma or aggressive, rapidly spreading lesions.
Where to source: curaderm.net (ships internationally). Also available: Curaderm BEC5 → Buy on Amazon
Boswellia sacra and related species have been used medicinally for centuries. Modern research is beginning to substantiate some of its traditional uses.
A 2024 study at MUSC's Hollings Cancer Center found statistically significant reduction in tumor proliferation with Boswellia extract compared to untreated controls. A 2013 published case report documented BCC resolution with topical Boswellia sacra essential oil application, with no side effects.
The FDA lists Boswellia gum resin as Generally Recognized as Safe.
Honest assessment: The clinical evidence for skin cancer specifically is limited — a small number of studies and case reports. This is appropriate as an adjunct alongside proven treatments, not a stand-alone primary treatment for anything aggressive.
Find Boswellia → (affiliate links coming soon)
Low vitamin D status is consistently associated with worse outcomes in melanoma across multiple published studies. Vitamin D plays a documented role in cellular differentiation and immune regulation.
Most people are deficient. Most oncologists don't check levels. This is a low-cost, low-risk area worth addressing.
What to do: Ask your physician to test your 25-OH vitamin D level. Work with your doctor to optimize it — generally in the 60-80 ng/mL range is what integrative oncologists target. Supplementation with D3 + K2 is typically used; K2 supports appropriate calcium metabolism at higher D3 doses.
Mistletoe extract (Viscum album) is among the most widely used complementary cancer treatments in Europe — particularly in Germany, Switzerland, and Austria where it is prescribed by conventional oncologists. Multiple meta-analyses document improvements in quality of life and immune function during conventional cancer treatment.
It is administered by injection and requires an integrative oncologist.
Find a practitioner: Society for Integrative Oncology — integrativeonc.org
At doses achievable only through intravenous administration, vitamin C acts as a pro-oxidant — generating hydrogen peroxide selectively within cancer cells through a different mechanism than oral vitamin C. Used at integrative oncology centers as an adjunct alongside conventional treatment.
Emerging clinical trial data is building. This is not a replacement for conventional treatment; it is used in combination.
Find practitioners: Riordan Clinic provider directory — riordanclinic.org
What the research actually says — not what social media says
A 2022 peer-reviewed study in Frontiers in Oncology found that oral ivermectin may help prevent melanoma metastasis by abrogating neutrophil extracellular traps. This is a legitimate published finding about metastasis prevention — not treatment of primary tumors.
Topical ivermectin cream (Soolantra) is FDA-approved for rosacea. There are no controlled clinical trials supporting its use as a primary treatment for skin cancer lesions. Some patient communities combine it with niacinamide topically; the niacinamide has strong published data while the ivermectin for primary tumor treatment does not.
Bottom line: The metastasis prevention research is worth watching. As a primary topical skin cancer treatment, the evidence does not currently support it. Do not substitute it for proven treatment.
We include this because people use it. Read the full picture before considering it.
Black salve is a topical escharotic made from bloodroot (Sanguinaria canadensis) and often zinc chloride. It causes tissue death — an eschar forms, sloughs off, and is intended to take the cancer with it.
Active patient communities report using it. The FDA considers it dangerous and has banned its marketing as a cancer treatment. Here is what the published research actually shows:
Lab studies confirm cytotoxic activity from the active ingredients. However, a large 5-year Australian histopathology study found cancer persistence in many black salve-treated lesions — meaning the surface appeared healed while cancer remained beneath, now potentially harder to detect and treat. Published case reports include serious scarring and at least one recent hospitalization.
If you are considering this:
- Do NOT use it for melanoma under any circumstances
- Do NOT use it as sole treatment for any aggressive or spreading lesion
- This should only be explored in consultation with a physician
- Clearance must be confirmed by biopsy — not visual inspection
- Document everything with dated photographs
We are not recommending this treatment. We are documenting that it exists, who uses it, and what the risks are — because you will find it in patient communities regardless, and we would rather you have accurate information.
📖 Want the Complete Protocol?
"Skin Cancer Diagnosis: What You Need to Know"
The deep-dive guide — specific protocols, dosing, what to ask your doctor, and the complete recurrence prevention plan. 40 pages, evidence-backed, written for patients not doctors.
"This is the resource I wish existed when I was first diagnosed."
Clinical Trials
This Is Not a Last Resort
Clinical trials give patients access to treatments not yet widely available — including options that may ultimately prove superior to current standard of care. Many trials are available as first-line options for specific diagnoses. Many cover the cost of treatment.
Ask your doctor at your first appointment: "Am I eligible for any active clinical trials?"
Where to Find Active Trials
- FreeClinicalTrials.com — filtered for skin cancer; easy to search by condition and location
- ClinicalTrials.gov — comprehensive federal database; search by condition, stage, and ZIP code
- Melanoma Research Foundation — melanoma.org/clinical-trials
- AIM at Melanoma — aimatmelanoma.org
What to Ask About Any Trial
- What phase is this trial?
- Is there a placebo arm — and what is the probability I receive it?
- What is the experimental treatment being tested?
- What are the known risks?
- What are the time and travel commitments?
- Are treatment costs covered?
Getting a Second Opinion
Every Patient Should Get One
Skin cancer treatment recommendations vary significantly depending on who you see. A general dermatologist, a Mohs surgeon, a radiation oncologist, and a melanoma specialist at a major cancer center may offer meaningfully different recommendations for the same diagnosis. The best physicians expect and encourage second opinions.
Remote second opinions are available from every major cancer center. You provide your pathology report and slides; they review and respond. Typically takes 1-2 weeks. Often covered by insurance; sometimes $300-500 out of pocket.
Top Centers for Skin Cancer
| Center | Location |
|---|---|
| MD Anderson Cancer Center | Houston, TX |
| Memorial Sloan Kettering | New York, NY |
| Mayo Clinic | Rochester / Phoenix / Jacksonville |
| Dana-Farber Cancer Institute | Boston, MA |
| UCLA Jonsson Cancer Center | Los Angeles, CA |
| Moffitt Cancer Center | Tampa, FL |
| Stanford Cancer Center | Palo Alto, CA |
Remote Second Opinion Contacts
- MD Anderson: mdanderson.org/patients-family/diagnosis-treatment/ask-md-anderson.html
- Mayo Clinic: mayoclinic.org/appointments/second-opinion
- Memorial Sloan Kettering: mskcc.org/experience-msk/becoming-patient/seek-second-opinion
Finding the Right Specialist
- Mohs surgeon: mohscollege.org/find-a-surgeon
- Integrative oncologist: integrativeonc.org
- Melanoma specialist: melanoma.org
Questions to Bring to Your Doctor
Print this. Bring it to your appointment.
Before Deciding on Any Treatment
- What is my exact diagnosis — type, stage, Breslow thickness (if melanoma), and margin status?
- Am I a candidate for Mohs surgery?
- Am I a candidate for Image-Guided SRT?
- What are all of my treatment options — including ones you don't personally offer?
- What is my risk of recurrence with each option?
- What happens if I take 30 days before deciding?
- Are there active clinical trials I should consider?
- Do you recommend I seek a second opinion at a major cancer center?
- What would you recommend if this were your family member?
💡 Print this page (Ctrl+P / Cmd+P) and bring it to your appointment.
Before Any Surgery
- What are your personal cure rates for this specific procedure?
- How many of these procedures have you performed in the last 12 months?
- What are the cosmetic implications, and are there less invasive alternatives?
- Will you test margins during surgery?
For Melanoma Specifically
- What is my BRAF mutation status?
- Do I need a sentinel lymph node biopsy?
- Which immunotherapy protocol do you recommend, and why that one?
- Should I be referred to a dedicated melanoma oncologist?
Prevention & Monitoring
The Single Best Thing You Can Do After a Skin Cancer Diagnosis
If you've had one skin cancer, your risk of developing another is significantly elevated. The highest-leverage, lowest-cost intervention backed by peer-reviewed clinical data:
Oral niacinamide — 500mg twice daily.
Vitamin B3. Available without a prescription at any pharmacy for approximately $10-15 per month. Supported by a Phase 3 NEJM trial and a 2025 JAMA Dermatology study showing up to 54% reduced risk of new skin cancer in high-risk patients.
Discuss with your physician before starting. It is a well-tolerated supplement, but your doctor should know what you're taking.
Know What Pre-Cancer Looks Like: Actinic Keratosis
Actinic keratosis (AK) is a pre-cancerous skin lesion caused by years of UV exposure. Left untreated, AKs can progress to squamous cell carcinoma. Knowing what they look like helps you catch them early.
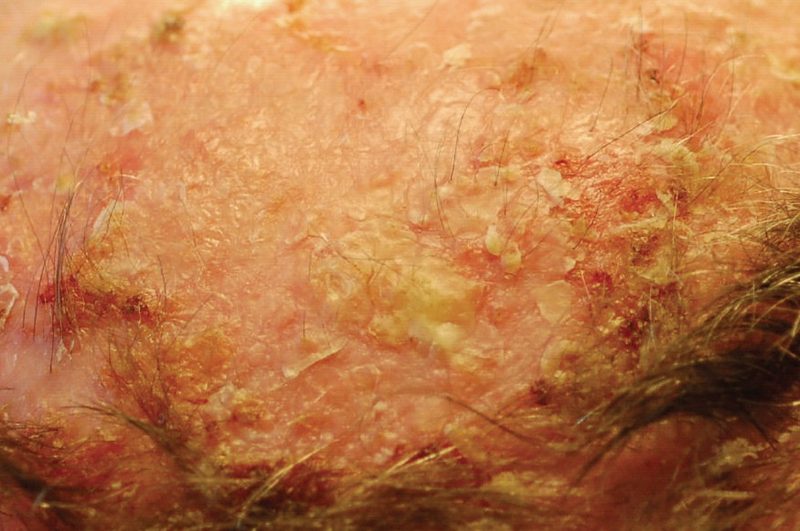
AKs typically feel rough or sandpapery to the touch, are pink to red in color, and appear on chronically sun-exposed areas: scalp, face, ears, backs of hands, forearms. Show any suspicious rough patches to your dermatologist — they're easily treated when caught early with cryotherapy or topical creams.
Sun Protection
- Mineral sunscreen zinc oxide → Buy on Amazon — SPF 30+, reapplied every 2 hours when outdoors
- UPF-rated clothing — Coolibar, Solumbra, and Mott50 make quality options
- Wide-brim hat; UV-blocking sunglasses
Monthly Self-Exam: The ABCDE Rule

- Asymmetry — one half doesn't match the other
- Border — irregular, ragged, or blurred edges
- Color — more than one color in a single spot
- Diameter — larger than 6mm (pencil eraser). Melanoma can be smaller.
- Evolving — anything that's changing: size, shape, color, or new symptoms
New or changing lesion? See a dermatologist promptly.
Annual Full-Body Skin Exam
Once per year minimum with a board-certified dermatologist. More frequently if you have a history of melanoma or multiple BCC/SCC diagnoses.
We update this page as new research emerges.
Enter your email to be notified when treatment options are added or updated.
We will never sell your email. We are not affiliated with any pharmaceutical company, treatment provider, or medical institution.
You're Not Alone
Patient Organizations
- Skin Cancer Foundation — skincancer.org
- Melanoma Research Foundation — melanoma.org
- AIM at Melanoma — aimatmelanoma.org
- Merkel Cell Carcinoma Resource — merkelcell.org (University of Washington)
- Cancer Support Community — cancersupportcommunity.org — free programs and support groups
- American Cancer Society — cancer.org — 24/7 helpline: 1-800-227-2345
Patient Communities
Real patients. Real experiences. Unfiltered.
- Reddit r/melanoma
- Reddit r/skincancer
- Facebook: "Melanoma Support Group"
- Facebook: "Skin Cancer Warriors"
Why This Page Exists
A Phase 3 NEJM trial proves a $10/month vitamin B3 supplement cuts new skin cancer rates by up to 54% in high-risk patients. Your dermatologist almost certainly never mentioned it.
A surgery-free radiation treatment with a published study of nearly 3,000 lesions shows cure rates matching surgery. Many patients are never offered it.
A topical vitamin C preparation outperformed a prescription cream in a randomized controlled trial. Almost no one has heard of it.
None of these are secrets. They're just not profitable to promote.
PlanetCure exists because patients deserve to know everything — not just what's most profitable to tell them. We cover what the system won't, we rate the evidence honestly, and we let you decide.
We are not telling you to skip your doctor. We are not telling you any single treatment will work for you. We are giving you the information you need to walk into your next appointment as an empowered, informed patient.
You deserve that. Everyone with this diagnosis does.
We update this page as new research emerges.
Enter your email to be notified when treatment options are added or updated.
We will never sell your email. We are not affiliated with any pharmaceutical company, treatment provider, or medical institution.
Disclosure: Some links on this page are Amazon affiliate links. If you purchase through these links, PlanetCure may earn a small commission at no additional cost to you. This does not influence our recommendations — we only link to products mentioned because of their evidence base, not for commercial reasons.
The content on this page is for informational and educational purposes only. It does not constitute medical advice, diagnosis, or treatment recommendations. Individual results vary and no treatment is effective for every patient or every diagnosis. Always consult a qualified, licensed healthcare professional before making any medical decision. PlanetCure is not affiliated with any pharmaceutical company, hospital system, or treatment provider, and does not receive compensation for the treatments or products mentioned on this page except where explicitly noted as affiliate links.